- By JANET ROCHE & CAROLYN ROBBINS
- Edited by David Goodman
- Guests: Mary Jo Cooper & Adrienne Jones Erdman
- Photo courtesy of: Bay Cove Human Services
• Mary Jo Cooper and Adrienne Jones Erdman join us to discuss designing a small group home for developmentally challenged individuals. As a result of living longer due to modern medicine, these individuals are also presenting with Alzheimer’s and Dementia. We’ll explore how evidence-based design can be used to solve behavioral issues that can arise in this type of group home, and in this particular case, how these design changes had an even greater impact than expected.
Topics in this episode include: Alzheimer’s, dementia, lighting, acoustics, preventing accidents, hoarding, and health professional design.
Mary Jo Cooper is the Vice President of Long Term Support Services at Bay Cove Human Services, Inc., a multi-service agency focused on disability services throughout the Greater Boston Area. She is responsible for the Residential, Day, Employment, Family, and Independent Support contracts that include over 50 different programs serving 800 individuals and their families. Mary Jo is involved in several committees and panels on Industry Standards, Trends, and Best Practices and is on the Board of Directors of the Massachusetts trade Association of Developmental Disability Providers. In addition, she has presented at conferences on a variety of topics including how the built environment can and should be considered an integral part of any treatment philosophy.
Adrienne Jones Erdman, MDS works as a Principal Human Factors Engineer with Cambridge Consultants in Boston, MA, where she facilitates the design of medical devices and equipment to fit users’ needs, capabilities, and limitations. Adrienne is a graduate of the first class of the Master of Design Studies in Design for Human Health program at Boston Architectural College and uses skills gained in the program to better understand the reciprocal relationship between products and the built environment. She has presented for the Human Factors and Ergonomics Society (HFES) and Environments for Aging Conferences and is a member of the American Society for Healthcare Engineering and the Center for Health Design.
Mary Jo Cooper email: mcooper@baycove.org
Adrienne Jones Erdman email: adrienne.erdman@cambridgeconsultants.com
References: Design details pdf- Bay Cove Presentation
Designing for: Developmental Disabilities & Alzheimer’s
Guests: Mary Jo Cooper & Adrienne Jones Erdman
(Music)
Janet: In this series we will be discussing specific examples of design techniques that can make a positive difference for people living with certain human conditions.
Carolyn: The more a designer understands the client and or the community the more effective and respectful the design will be.
(music up, then lower)
Carolyn: Evidence based design can be an important part of designing for behavioral issues and sometimes, it can even help solve them.
Janet: We recently had an opportunity to sit down with Mary Jo Cooper and talk about a situation in a group home that was not only disturbing to the residents and staff but also to the neighboring community. Adrienne Erdman and I worked as a part of the inclusive design team on this project.
Carolyn: Before we get to that discussion, let me tell you a little bit about our guests and their qualifications:
Mary Jo Cooper is the vice president of Long-Term support services at Bay Cove Human Services Incorporated. A multi service agency focused on disability services throughout the greater Boston area. She is responsible for the residential, day, employment, family and independent support contracts that include over 50 different programs serving 800 individuals and their families. Mary Jo is involved in several committees and panels on industry standards, trends and best practices and is on the board of directors of the Massachusetts trade association of developmental disability providers. In addition, she has presented at conferences on a variety of topics including how the built environment can and should be considered an integral part of any treatment philosophy.
And today we also have Adrienne Erdman who works as a principal human factors engineer with Cambridge Consultants in Boston Massachusetts where she facilitates the design of medical devices and equipment to fit users needs, capabilities and limitations. Adrienne is a graduate of the first class of the Master of Design Studies in the Design for Human Health program at the Boston Architectural College. She uses the skills gained in the program to better understand the reciprocal relationship between products and the built environment. Adrienne has presented for the Human Factors and Ergonomics Society and Environments for Aging conferences. And she’s a member of the American Society for Health Care Engineering and the Center for Health Design.
Janet: In today’s discussion we are examining how evidence-based design can be used to solve the behavioral issues that can arise in a group home. And in this case how these design changes had an even greater impact than expected.
Carolyn: As someone who is just learning about the field of designing for living conditions, I was very impressed with the outcome design had in this situation. See if you agree.
(Music- Transition to Interview)
Janet: Welcome ladies. Welcome to Inclusive Designers podcast. Mary Jo, why don’t we start with you. (OK) Mary Jo you were the impetus for this particular project, and you saw the benefits of using designers to solve a problem that you were experiencing within one of your residential homes. Can you speak to a little bit about that…
Mary Jo: Sure. We had built a home in the early 2005 area and it was built specifically for people that had major medical issues that were coming from nursing homes and needed a lot of medical support. And it was great. It worked perfectly. Well over the years, people started to age and had regular complications of aging. But also, there was a lot of dementia in the house. So, the house had four people living in it. And what was happening is everybody’s dementia presented in a different way. Including one woman who was just, she had a lot of terror and would scream quite a bit, and part of her communication was screaming. And it was upsetting to not just the people that lived in the home but also to the neighbors. So, at that point we really wanted to make sure that people could stay in their own home, but we wanted the home to then work better for them. So I started doing some research and looking around and I couldn’t quite figure out who the experts were for this and was making all kinds of calls and finally wound up talking to some lady in Minnesota I think who said ‘gee right there in Boston you’ve got this design for human health program and Dak Kopec is the director and he is kind of the expert you should really just call the guy down the street’… And that’s how I kind of connected.
Janet: I did not realize that that was the connection. That’s fascinating. So, speak a little bit further about the resident that was vocalizing and without using names because our particular conversations due to HIPAA laws and we really want to keep people’s medical information sacred and confidential.
Carolyn: It’s more about the situation, in other words, than the name.
Janet: Correct. Right. So, speaking to that topic can you explain a little bit further what the actual issues were within that modular home?
Mary Jo: Sure. So, there were four people living in the home and this one woman in particular who was doing a lot of vocalizing. Her bedroom was right off the living room and her windows looked right onto the street, and it was a very active street with a lot of people outside all the time, there was a park, there was all kinds of stuff. And she would, she didn’t really talk much, she would vocalize to most of her communication kind of in a guttural way. As she got more and more demented, she was, these vocalizations were getting much, much louder.
Janet: Was she Sundowning, do you think. (Probably). And what is Sundowning, can you explain…
Mary Jo: Sure. So, as people are going through a different phase of dementia there are different symptoms that show up. And particularly as light changes, symptoms change. And so sundowning typically is referred to as a time of day when people’s symptoms increase. and it can be different for different people but most often it’s late afternoon early evening. And so, at those times she would be much more vocal and much more agitated. And for some reason she got a lot of strength behind her vocalizations so she was really loud. Even if she wasn’t in terror, even if she wasn’t in pain, if she was just communicating, she just, her, the way she communicated changed. And it did upset people living with her, because it was scary if they didn’t know what was happening or if she was OK even if they were looking at her. She couldn’t tell them that she was OK or what was happening. And people outside had no idea what was going on. So, they were calling the police they were saying we were abusing her, that other people that lived in the house were abusing her and that wasn’t the case at all. It was just that she was communicating in a very loud way.
Janet: Being a part of the project, I know that when we got there, there were certain design elements from the modular home that were a factor and creating problems within the community and within the walls of the residence itself, and then obviously with the workers. Can you speak to us a little bit about some of the design issues at that point that we then, we will talk about later and how we fix those, but maybe you can set up for our listeners a little bit about what the modular home looked like.
Mary Jo: Sure. So, it’s a four-bed home and it’s, you go in, it’s a typical ranch I guess is what you would say. So, you go right in the front door which is right into the living room. And immediately on that first wall as you walk in on the left was the door to a bedroom and in front of you is the kitchen. But it’s all open. You go then around down ahall where there are three other bedrooms and two bathrooms as well as sort of an open area that leads out to a pretty nice deck that overlooks the park. And that’s where we had kind of our nurse’s medication area.
Janet: For those of you who are listening, you don’t know, we are in Boston so, the greater Boston area. And as a result, so when you open up the door those can be problematic during the winter and the elements then find their way into this residential home.
Mary Jo: Sure, so the outside was part of the environment as well because if you open the door there was a ramp, you open the door and you’re right outside. And so, if it’s cold out all that cold air was coming right in. If it’s raining out, the rain can come in. And on the other side of that in the summer when it’s warm and there are lots of kids and people outside, we had quite an active neighborhood where everybody could hear everything if the windows were open because they’re right there.
Janet: Right, anything else you want to add to describe the design and maybe the design problems that (sure) were a contributing factor or maybe perhaps there were design issues that were just born out of the particular type modular home that you guys had…
Mary Jo: Sure, a couple of things. one is, we had built the house so that most of the people could leave the home by bed, so that we weren’t having to transfer people from bed to wheelchair then out. It saves time and because of our funding, we need our funding regulations and just common sense you need to get people out within two and a half minutes if there’s a fire (right or some sort of emergency). So, three of the bedrooms actually had, (Janet: Two…) two of the bedrooms have French doors in them where people could then wheel the beds directly out. Two did not, but were very close to doors. The floors were hardwood. (Mm hmm). which, they were lovely. (Right.)
Janet: … but acoustically for vocalization, for Sundowning and what have you.
Mary Jo: And got really slippery.
Janet: Oh, and got slippery, yes of course. Right.
Mary Jo: And you know, it’s a group living environment so that, we had three different shifts of staff coming on, those floors were getting washed three times a day because we had all kinds of people walking around and body spills and different things happening and so they were getting washed three times a day, and that’s tough on a hardwood floor. The windows were just regular windows.
Janet: Single pane, weren’t they? or there will be maybe double pane, Right?
Mary Jo: Yeah. And the, because it was a modular home, the walls weren’t particularly thick or insulated in a way that was anything fancy, it was just sort of regular built.
Janet: Right.
Mary Jo: So those were those were some of the issues that that did kind of play into some of these things. Also. I think the lighting wasn’t terrific.
Adrienne: Yeah. The one room with the woman who was vocalizing, I remember it was particularly dark and she had a very, it wasn’t hot pink because that says bright to me. But it was (bubblegum). Yeah, bubblegum pink. It was yeah but it was like not helping the situation. It was very dim in her room in particular.
Janet: It was weird, because it was dim, but it was also extremely bright and powerful. A.J. – maybe you can talk now, maybe this is a great way to segment into sort of what we did in terms of research… because that particular room in itself, that was the room for the resident who was doing the vocalization and it had some, she was right smack dab in the middle of the actual residence itself. She had these hot pink walls, (Mary Jo: which was her choice) which was her choice, and we get into in a minute sort of what we did in order to appease her but yet bring down the hotness of the room. And then again, it was about acoustics and lighting and so on and so forth. So, but Adrienne maybe you can take us through a little bit about how we did the research and what we did and kind of go from there.
Adrienne: Sure. So, once we heard this project brief from Mary Jo, we set up some time to do site visits at the home and I think we did a few in total across, we had a team of three, so across all of us. And although this one resident was vocalizing and it was causing issues in the neighborhood and causing issues with the staff that became the primary concern, but we can’t forget that there are three other people living there and an entire staff that works there. So, our first objective was to understand all of the other people, all of the other players, in this space, because they have needs too, and we wanted to be sure that we designed according to those needs. So, within the three other residents, this one woman was in, or she was ambulatory, right. And there was another woman who’s in a wheelchair. And then there’s a third woman who was probably relative to everyone had the most violent Dementia behaviors. I think there was an incident with (knives) knives and getting into cabinets with knives that she shouldn’t have. There were other issues with hoarding towels, and kind of hiding stuff within her room.
Janet: And these are all very indicative behaviors of people, right, who have some sort of form of dementia.
Adrienne: Exactly. And then there is a fourth resident who is a male who we wanted to learn about him as well and so he had, was it Down syndrome, yeah. And loved the Red Sox. So, we went through this whole process of understanding these other people in terms of their personal interests and also their, whatever conditions they have and how those conditions manifest.
Janet: One of the things that we do as designers for ‘design for human health’ is to look at the biology, psychology and sociology… So, you know, he was a great example of kind of looking at all that in order to design correctly for him.
Mary Jo: And also, he had, he also had the very early stages of dementia showing.
Adrienne: Which is a good point. They were all like along a spectrum right. They all had kind of different symptoms at the same time so we had to figure out how to balance all of that. And so, when we looked at the biological, sociological and psychological factors. So that was based on the different conditions because you know that changes how you interact with the world and changes how you perceive things. And that’s not how we experience the world. So, we had to go and do a lot of scientific literature searching to understand how each of these conditions manifest in each of those three different ways and then try to pinpoint where the commonalities, where the specific things that each person needs because that helped us to identify what is the living room need. What is resident one’s room need different from resident two, and so on and so forth. So that helped us really tie our ideas to specific needs. And separately with the site visits we thought it was really important to talk to the staff and I remember at the end they were very thankful that we considered them, they you know they’re very selfless like caring people and didn’t think of themselves as residents in the home but they are. It’s 24-hour nursing. All of the residents are dependent on them for all of their activities of daily living which are things like dressing, bathing, eating, etcetera. So, we wanted to understand like what do you need to do to do your job. What do you need to do to feel safe in this home. Do you need to lock up your belongings, like what do you do now, why is it not working and go through all of the details. So, we definitely spent a lot of time upfront trying to gather all of that information and then sort it out and try to see where those themes in those common points were.
Janet: Right. Yeah. it was a great undertaking and you did most of the research and I took care of the F-F-and-Es— for those of you that don’t know it’s furniture and fixtures and equipment— and, but it was a great collaboration I thought and I would like for you now Adrienne to kind of speak a little bit about some of the findings that you came up with and then maybe Adrienne you and I can talk a little bit about some of the design elements that we came up with. And then Mary Jo bring it home to tell us how everything’s going.
Adrienne: Sure. So, I think one of the biggest things that we found through the research that we did for individuals with dementia is that you need to facilitate ‘way finding’ a lot more than you would a typical population. So, there’s a lot of research out there about case studies where people have wandered out of their homes and wandered off into neighborhoods and kind of get lost because of some issues finding their way back home. So, we knew that of these four residents we needed to help them identify their rooms in a way that was meaningful for them and so we did that through color. And we, I think, were kind of inspired by the hot pink walls…
Janet: we were inspired by the hot pink walls…
Adrienne: And the fact that she picked that color out we thought you know that’s important we don’t want to take that away from her because that’s her, what she loves. That’s an individual choice. And so, we decided we would do something special for the other three residents as well. And but to tone it down a little bit we made three of the walls of her room white and then there was one accent wall that was pink and that really helped with the dim situation, in addition to some lighting, and helping bring some more brightness into this space. To match that on the door, so it’s a four or six paneled door, just like a very typical door. And the bottom two panels we actually had suggested to paint a color to match that accent wall. So, we’re building a little bit of a theme for each resident you know. That’s the pink room, that’s green room etc.
Janet: And blue. And then we also had purple.
Adrienne: And then we had the sound panels…
Janet: And the sound panels too. We had everything kind of matching for each of the individual residents. But to, back to just kind of backtrack a little bit here we put the colors at the bottom of those panels on the door. Do you want to speak a little bit about that and why we did that, even though the woman that was vocalizing who had the hot pink room she was in a wheelchair, but it was still a way for her to identify her room and knew that she was going into her room and her space.
Adrienne: Right. So, and that’s a good point because even though it was specific to these four residents at the time, we knew that the design elements we put in needed to be adaptable to future residents as well, so, within that home and other homes. So, we did the two lower panels because of it having improved visibility. When someone is older and with developmental disabilities they tend to look down more when they walk. And so, it’s kind of akin to having something at eye level. You know in a museum for example you want something at eye level so with this population because they’re more inclined to look downwards when they walk, it needs to be, follow suit with where their eye level is now at.
Janet: Right. And you know and to that point you know it’s about them also shuffling. So, let’s keep moving on with the different types of design elements that we came up with. So, if you could also talk a little bit about acoustics and or you and I can talk a little bit about the acoustics which really, I think helped quite a bit.
Adrienne: Yes, so in addition to that each of the sound panels in each room and so each of those sound panels had an image on it. She can make it look like artwork. And so that was individualized for each room. We also had some more generic ones within the living room and elsewhere within the home. And we also suggest suggested putting in three paneled windows so the thicker material essentially helps mitigate against any sound that’s happening within the home.
Janet: And to double it up we also suggested acoustic (curtains) curtains. Thank you.
Adrienne: One of the other big things that we found to help with this hoarding behavior. So, we actually learned that the violent outbursts and the hoarding can have a connection. And it’s basically due to the fact that someone who has dementia, they can’t remember where they put things so if they can’t see it it’s not there someone stole it and I’m going to go get it. And so that is what caused stealing the towels. There also are issues with people being able to flush things down the toilet. So just trying to hide things for themselves and it kind of goes into this paranoia state. And so, one of the things that we found is that actually some level of open shelving helps mitigate against that because…
Janet: I thought that was a really important part that actually worked really well. And it’s also something that I, my mom has Alzheimer’s, and something we did with her was to show how these open-air kind of you know closets and bookcases and stuff like that for her stuff because she kept thinking that it was wandering off and it just ,right, it wasn’t, right. So, if she could see it she knew where it was. Everything came out from all the closets.
Adrienne: Exactly. So, then it helps the staff have more privacy with their belongings and so it kind of helps feed that need as well.
Janet: Right. Terrific. Mary Jo would you like to speak a little bit about sort of the aftermath of some of the design implications that you put in. Real quick, what particular designs did you actually put in and then what were the outcomes for these particular elements.
Mary Jo: So, the outcomes have been terrific. We did do quite a bit. We did put more carpeting in instead of all hardwood which helped. The nurses didn’t want to do all carpeting because there are some hygienic issues. But having some carpeting did really help quite a bit. The windows were huge and not just for the sound but also the insulation and for a whole host of reasons (right). our heating bill went quite down this year. We put an awning over the ramp. (Oh right.) That you know really helps with people coming in and out so that they’re, when they get off the van or wherever they’re coming from, work or day program, that they’re not out in the rain or the snow. And so, when they come in, it’s, the transition is much easier. It’s a you know it’s a nice transition and you’re not getting all the elements on the floor as you walk in or as you wheel in. We did, like Adrienne said, the colors have been terrific. We’ve done quite a bit with the open shelving and more open concept but also, I think Adrienne kind of circled this a little bit. The real person-centered planning, like really investing in what’s important to that person, what makes it home for them and building on that, so that each room then had a very different feel. So, the one lady who was very anxious and agitated, and was worried that people were stealing her stuff. She’s also from the south. She was quite a lady. Like a church lady.
All: She had a lot of hats and gloves. She was very fancy.
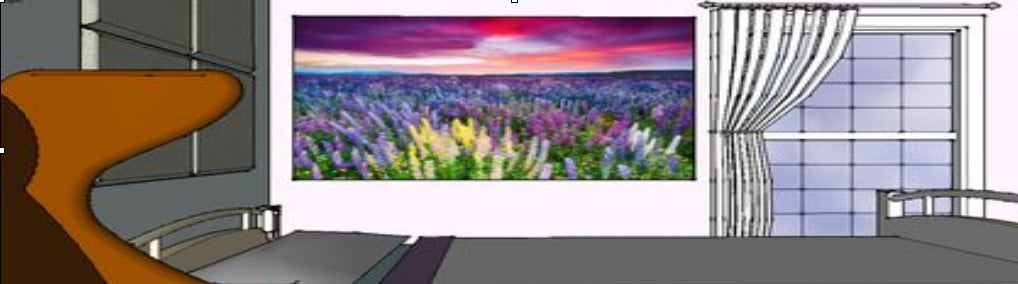
Mary Jo: But that really spoke to her. And so, and her sound panel was very particular. It was you know flowers in a field that was very comforting to her because that’s what she grew up with.
Janet: It was familiar, it was Southern looking, right.
Mary Jo: Whereas the gentleman who liked the Red Sox his sound panel was the green monster, (right) and he got the biggest kick out of that. (Right). So those elements that made it theirs are really important and it did impact people’s behavior.
Janet: Can you speak a little bit more to that… I mean, I know that the woman that was doing the vocalization, most of the vocalization had stopped… I mean that in itself is pretty much huge… can you speak a little bit to that and how did the community react.
Mary Jo: Well it got to be circular, because she would get agitated or she would start vocalizing, and then other people in the home didn’t quite understand what was happening because they were in their own kind of dementia path, and couldn’t remember from day to day necessarily, or vocalization to vocalization, that that she actually was OK.
Janet: Right. She’s been doing this every day right. Groundhog Day.
Mary Jo: Yeah. So, they would get more agitated, which would get her more agitated. And so, once we were able to kind of intervene and some of that, and people were able to sleep better because they weren’t hearing as much vocalizations because the, you know the sound panels, the flooring all those different things happened and actually having some better lighting that was able to, we were able to kind of track some of the Sundowning behaviors when it would start. And so, we couldn’t stop the dementia, but we could certainly work with it in a different way. And that I think was what happened.
Adrienne: I think you told me that afterwards that you had a barbecue with your neighbors.
Mary Jo: We did. Yeah.
Adrienne: I thought that was just amazing.
Mary Jo: Yeah. and actually, the neighbors…
Janet: because they went from calling the police to now having a barbecue right.
Mary Jo: Yeah. And the neighbors have been actually really lovely because we were pretty open about what we were doing. And what was happening in the home because people were terrified initially when we said we were gonna be putting a group home there. People automatically assume it’s gonna be you know a danger to the neighborhood and in fact it wasn’t but when there’s a lot of screaming and there’s a lot of, it does raise some concerns. Right.
Janet: Which goes back to almost the sociology of the particular space. And you know, a lot of the neighbors you know like you said they have the misconceptions and their misconceptions were actually by default becoming truthful in their head because there are people screaming but at the end of the day it wasn’t anything like that.
Mary Jo: It wasn’t like that right. And we were able to do a little bit of education and invite people in, invite the neighbors and to see what was happening and how things were going. and now the neighbors are big supporters and actually will come and talk to our staff about, ‘gee my aunt seems to be not kind of how she was what do you know about this and can…’ So, it’s actually been a nice way to do some of that stuff. We have had people, have since died and other people have moved in, and we’ve re- , you know kind of done the person-centered stuff so that their room is their room, it’s no longer for the person it was initially but it’s worked out lovely. Yeah. And so, we’ve changed out the sound panels or we’ve changed the colors, but it’s still it still works really nicely.
Carolyn: It’s very impressive. It really made a difference. I love this story and its ending and how it can be used for others as well.
Adrienne: Yeah, I think that’s a thing I would like to pass on to other designers is to be sure that you tell the full story that it doesn’t just stop at the design that you’ve suggested. You need to understand like, how did things change in a measurable way after you implemented the design. You know, that was hard for me in terms of finding research going in like, OK I have an idea of what the problem is and an idea for how to fix it, how do I know it will be effective. And it’s really hard to make that determination without some kind of data to follow up.
All: (Data to follow up). it’s really great that. (That’s important). That you’ve been able to provide some feedback.
Mary Jo: And one thing I would certainly add in is, one of the things Adrienne did that was so important was that she read all of our regulations because we are publicly funded. (Great point) we have to live by certain things. And it does impact design. And so, part of what Adrienne did was so important because it, she tied the regulatory stuff in with the medical and design pieces and the biology, sociology and psychology kind of all needed to fit together in terms of mission and vision and regulations.
Janet: Well this is a great place to end ladies, thank you so much for stopping by today at Inclusive Designers and hopefully I’ll have you guys on again. All right.
Guests: Thank you for having us.
Janet: Thanks guys.
(Music- Transition to Outro)
Carolyn: If you have any questions or have suggestions for future topics you’d like us to cover, shoot us an email: info@InclusiveDesigners.com
Janet: For more information on the design and research we cover, please check out our web page at: InclusiveDesigners.com.
Carolyn: and in case you didn’t get it, that’s InclusiveDesigners.com. We hope you enjoy our Inclusive Designers Podcast forum.
Janet: And we look forward to your feedback too.
Carolyn: Yes, we do. Thanks for listening.
Janet: Until our next podcast episode. Stay well… and stay well informed. Thanks for listening.
Carolyn: yes, thanks again.
(Music- up and out)